
Development of CURE-Elderly-Personas
The development process of CURE-Elderly-Personas consists of four steps:
- Defining AAL Requirements
- Matching Data with AAL Requirements
- Forming CURE-Elderly-Personas Skeletons
- Creating Text Content and Refining CURE-Elderly-Personas
Step 1 Defining AAL Requirements
The project partners started with an initial evaluation of national and international AAL (and related) projects. Results were categorized into target groups, project goals and applied technological approaches within the field of AAL technologies (see Figure 1). The font size represents the frequency of the topics the bigger the more often they were found in the project analysis. These findings constitute the topics of requirements needed to create the CURE-Elderly-Personas.

Figure 1: Overview on target groups, project goals and applied approach
Step 2 Matching Variables with AAL Requirements
For the generation of the CURE-Elderly-Personas SHARE data from the acquisition wave 1 was defined as data basis. This data material includes more responses than wave 2 and shows less missing data. Based on the results from step 1 the database was explored to identify scales and variables that may be used to form the CURE-Elderly-Personas. First descriptive statistical analysis outlined the characteristics and variations of the matching scales and variables. Since respondents in the age group 50 to 59 years show good health and marginal variations in the numerous variables related to health, the CURE-Elderly-Personas concentrate on persons aged 60 years and older. The result of step 2 was the definition of the main scales and variables that build the base for the CURE-Elderly-Personas (see Figure 2).
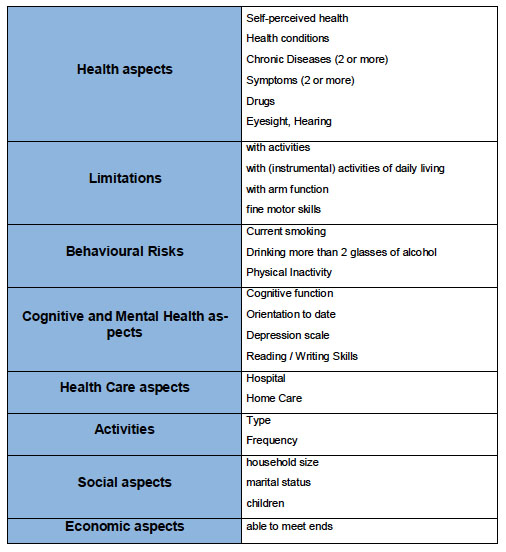
Figure 2: Variables that build the base for the CURE-Elderly-Personas
Step 3 Forming CURE-Elderly-Personas Skeletons
Cluster analysis was defined as statistical method to generate clusters that build the base skeleton of the CURE-Elderly-Personas. Since comparative studies indicate remarkable differences in health status and life expectancy across Europe (Vallin, Meslé & Valkonen, 2001) it was decided to divide the database into three groups: Germany and Austria (central European countries), Italy, Spain and Greece (southern European countries) and Sweden, Denmark and the Netherlands (northern European countries). Data from Switzerland was not included for the group of central European countries since the individual response rate in this country is very low (Börsch-Supan & Jürges, 2005) which might indicate problems for the representativeness of the Swiss sample. Results from cluster analysis could show that rather small variations between central, north and south European countries in the age group 60 to 79 years occur. More variation could be found in the age group 80 years and older. Thus, it was decided to generate 4 Persona sets one valid for central European countries (age group 60-79) and three sets each for central, northern and southern European countries (age group 80+) (see Figure 3).
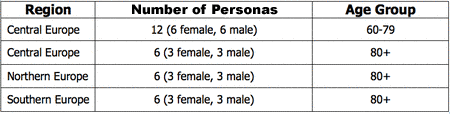
Figure 3: CURE-Elderly-Personas sets for different age groups and European regions
References:
Börsch-Supan, A., & Jürges, J. (Eds.) (2005). The Survey of Health, Ageing and Retirement in Europe Methodology. Mannheim: Mannheim Research Institute for the Economics of Ageing.
Vallin, J., Meslé, F. & Valkonen, T. (2001). Trends in mortality and differential mortality. Council of Europe, Strasbourg.
Step 4- Creating Text Content and Refining CURE-Elderly-Personas
In the final step statistical data were transformed into narrative textual descriptions that build CURE-Elderly-Personas. Since SHARE does not include information on technology usage additional data from different sources (e.g. market research, EUROSTAT) were used for shaping CURE-Elderly-Personas to get the Personas alive (details about data sources see in the CURE-Elderly-Personas manual). A visualization concept was applied for information based on SHARE such as household size, social contacts, income as well as cognitive and memory functions, diseases, symptoms and limitations to reduce textual information and to make statistical data more concrete. In a workshop with AAL designers and engineers the final CURE-Elderly-Personas were evaluated focusing on their understandability.
Acknowledgements
The CURE-Elderly-Personas are fictitious persons synthetically generated from average traits mixed across countries. Photos are taken from an external database. CURE-Elderly-Personas materials and documents do not represent private data from a single person. Information included in CURE-Elderly-Personas materials and documents do not infringe any privacy and data security rights.
This project website and project documents presented uses data from SHARE. The SHARE data collection has been primarily funded by the European Commission through the 5th framework programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life). Additional funding came from the US National Institute on Ageing (U01 AG09740-13S2, P01 AG005842, P01 AG08291, P30 AG 12815, Y1-AG-4553-01 and OGHA 04-064). Data collection for wave 1 was nationally funded in Austria (through the Austrian Science Foun-dation, FWF), Belgium (through the Belgian Science Policy Office), France, (through CNAM, CNAV, COR, Drees, Dares, Caisse des Deports et Consignations et le Commissariat General du Plan) and Switzerland (through BBW/OFES/ UFES). The SHARE data collection in Israel was funded by the US Na-tional Institute on Ageing (R21 AG 025169), by the German-Israeli Foundation for Scientific Research and Development (G.I.F.), and by the National Insurance Institute of Israel. Further support by the European Commission through the 6th framework program (projects SHARE-I3, RII-CT-2006-062193, and COMPARE, CIT5-CT-2005-028857) is gratefully acknowledged. CURE-Elderly-Personas materials and documents do not represent private data from a single person participated in the SHARE project.